Testosterone is a hormone that promotes the development and maintenance of male sexual organs, including the prostate.4 Testosterone is also implicated in a variety of prostate-associated diseases. One such disease is prostate cancer, which commonly depends on testosterone for its survival and growth.5,6
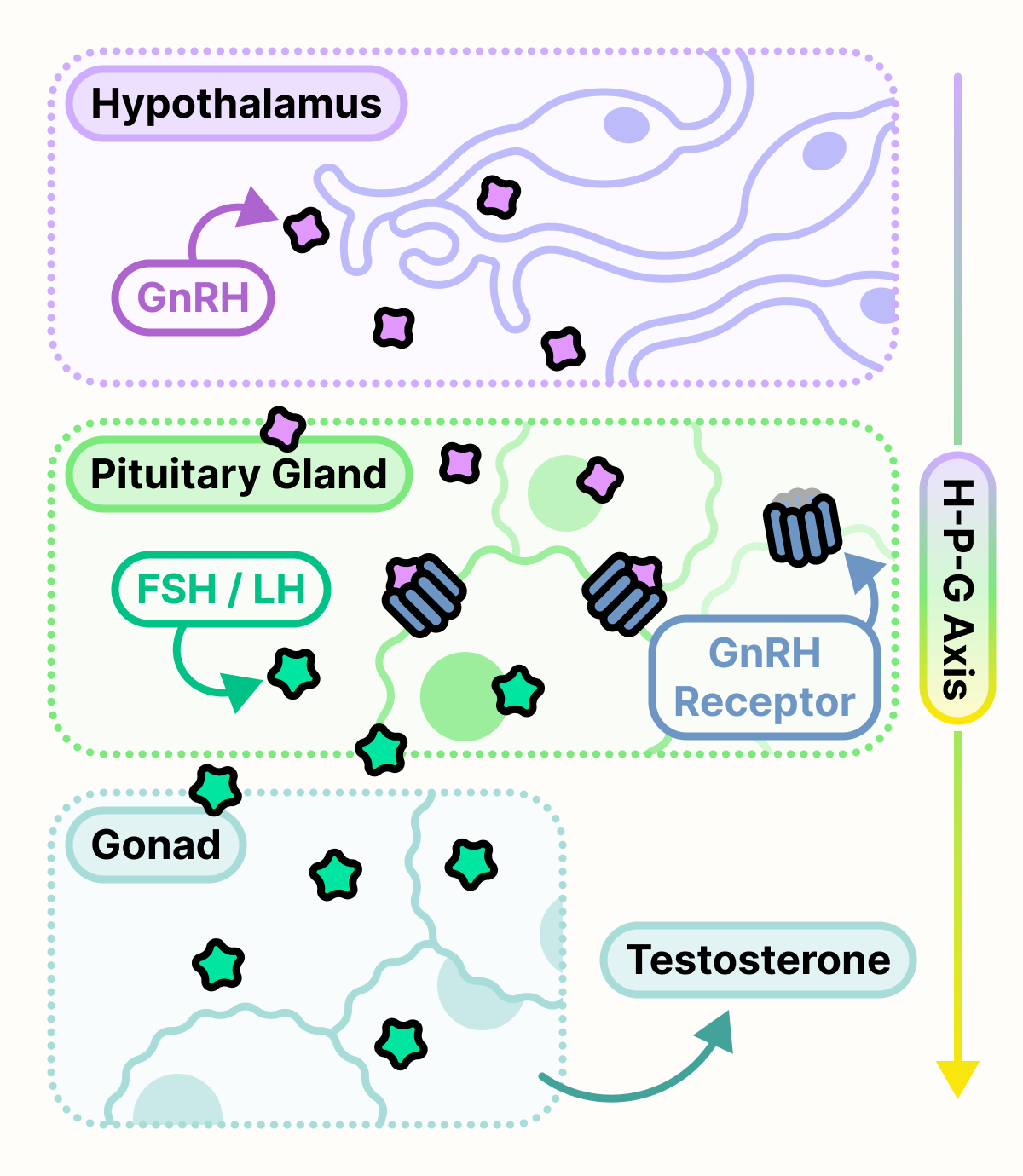
In our body, testosterone production is mediated by the hypothalamic-pituitary-gonadal (HPG) axis. This stepwise process begins with neurons in the hypothalamus of the brain, which release a hormone called GnRH. GnRH is transported to the pituitary gland where cells have GnRH receptors on their surface. When GnRH binds to GnRH receptors, these cells release a set of hormones called FSH and LH. FSH and LH is then transported to the gonad, in this case the testes, and stimulates the production of testosterone.7
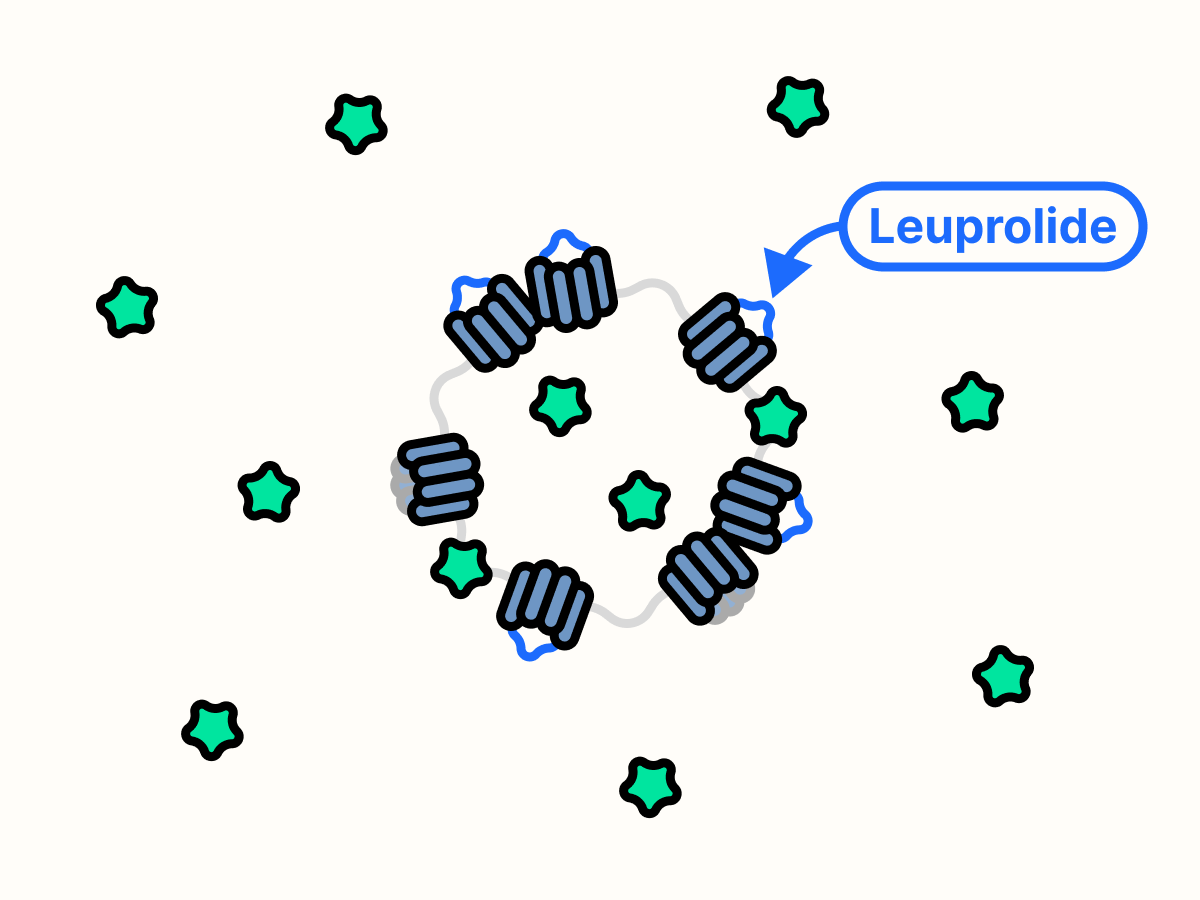
Because the HPG axis is the major source of testosterone in the body, blocking this axis can significantly reduce the testosterone available to prostate cancer cells.8 Somewhat paradoxically, the prostate cancer drug leuprolide is a GnRH analog that can bind and activate GnRH receptors. Just like GnRH, leuprolide initially stimulates cells in the pituitary gland to release FSH and LH, which drives testosterone production in the gonad.9
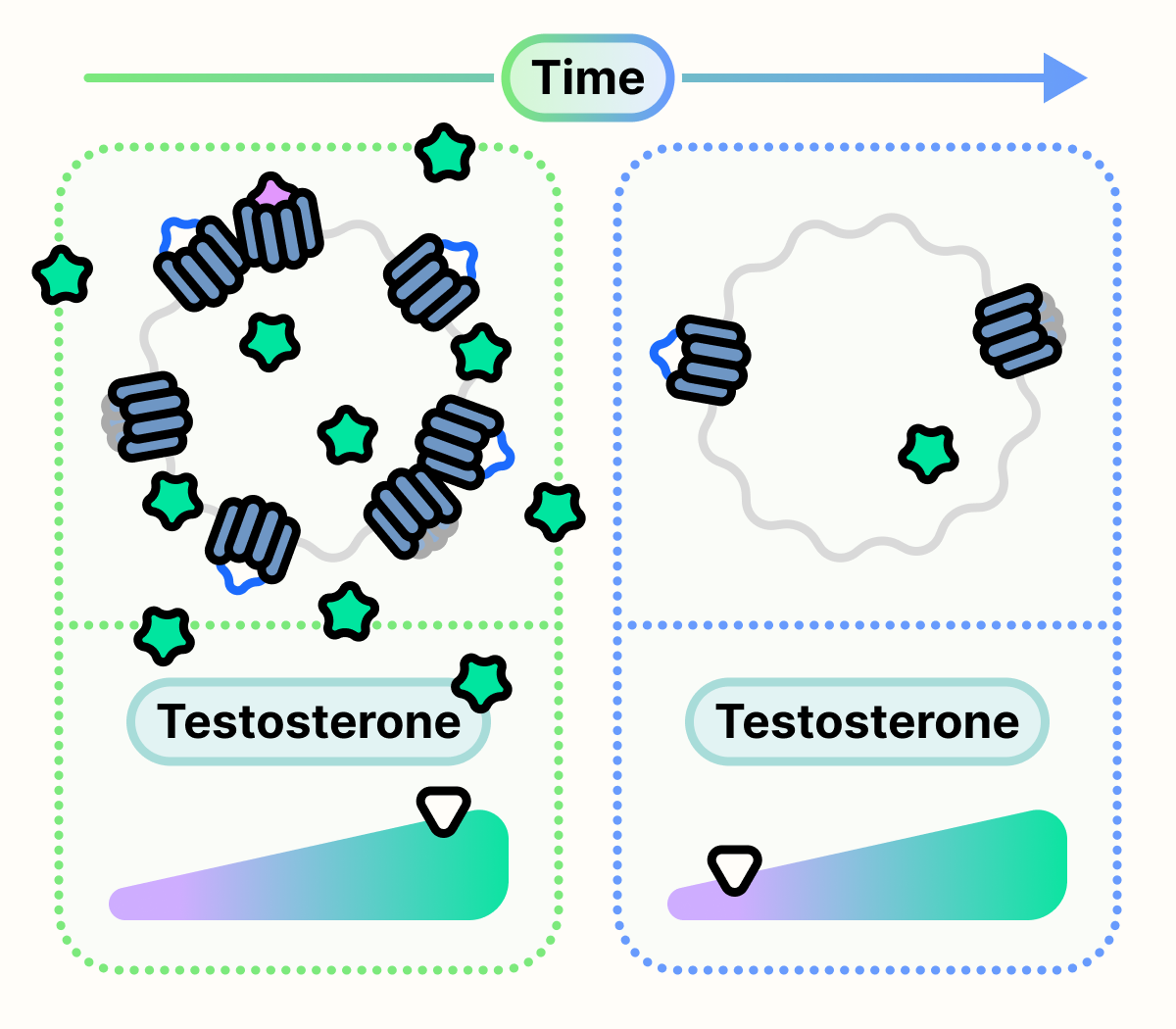
However, after continuous stimulation, the cells of the pituitary gland become desensitized to leuprolide and GnRH. This desensitization occurs due to the reduction of GnRH receptors present on the surface of the cell.10 This results in a significant decrease in FSH and LH, and consequently, testosterone production.
Ultimately, the depletion of testosterone halts the growth of testosterone-dependent prostate cancer cells and results in their death.11